Introduction
I’ve lost count of how many patients arrive at Phoenix Physio with pain on the back of their wrist and a story that goes something like this: ‘I thought it would just go away on its own.’ Sometimes they’ve been waiting three months. Sometimes six. And almost always, they wish they’d come in sooner.
Dorsal wrist pain is one of those conditions that looks minor from the outside. There’s no dramatic injury. No bruising. The condition manifests as a subtle ache on the back of the wrist, gradually intensifying to the point where it interferes with daily activities such as typing, going to the gym, and even picking up a cup of tea. Left alone, it doesn’t tend to get better. It gets more embedded.
In this guide, I want to give you a proper, honest explanation of what’s causing your dorsal wrist pain, what a diagnosis actually involves, and what treatment looks like at our Aylesbury clinic. Not a generic overview — a practical guide based on what I actually see and treat day to day across Aylesbury and Buckinghamshire.
What Is Dorsal Wrist Pain, Exactly?
‘Dorsal’ simply means ‘back of’—it’s the side of your wrist you see when your palms are facing down. When patients describe pain here, they usually point somewhere between the knuckles and the forearm, on the top surface.
The structures that most commonly cause trouble in this area are:
- Extensor tendons — these run from your forearm across the back of your wrist and are responsible for extending your fingers and wrist backwards
- Dorsal joint capsule — the connective tissue that wraps around the wrist joint itself
- Scapholunate ligament — a small but important ligament connecting two of the eight small carpal bones deep in the wrist
- ECR and ECU tendons — the tendons controlling side-to-side wrist movement and forearm rotation
- The carpal bones themselves — which can develop bony lumps or be strained by loading
Dorsal wrist pain tends to feel like a dull ache that sharpens with specific movements—especially bending the wrist backwards. You might also notice clicking, a visible lump, or weakness with grip. We’ll go through each of these individually.
Seven Things That Commonly Cause Pain on the Back of the Wrist (Dorsal wrist pain)
This matters because the treatment for each is different. Treating extensor tendinopathy the same way you’d treat wrist impingement is one of the main reasons people plateau in their recovery. Let’s go through each one.
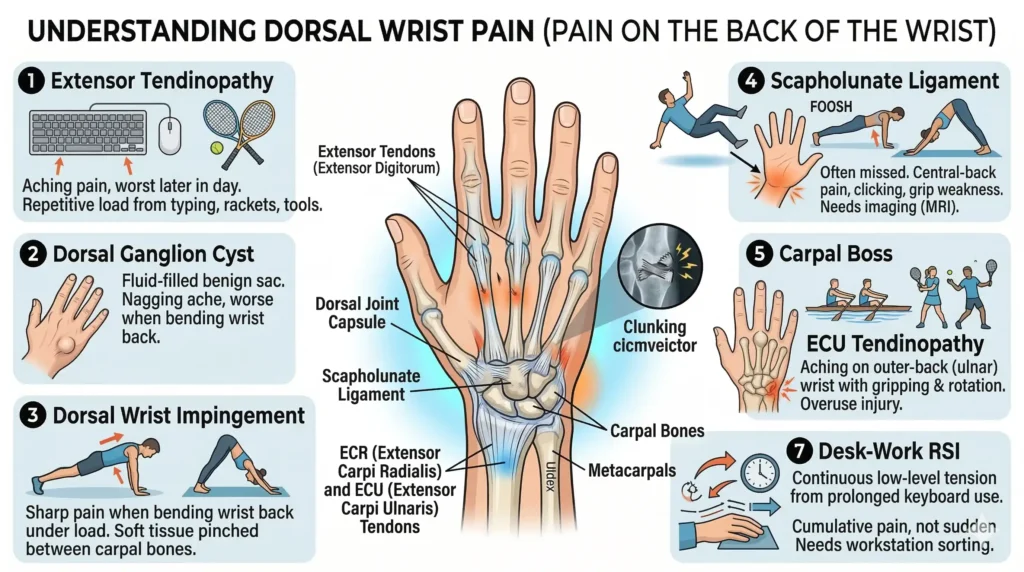
1. Extensor Tendinopathy
Honestly, this is the one I see most. The extensor tendons cop a huge amount of repetitive load — from typing, from tool use, from racket sports — and over time they stop coping with it. The result is a gradual build-up of aching on the back of the wrist. It’s usually worst later in the day and better in the morning. Ring any bells?
NHS data puts overuse tendon injuries at over 30% of all musculoskeletal GP consultations in working-age adults in the UK. So you’re in good company—but it does need proper treatment, not just rest and hope.
2. Dorsal Ganglion Cyst
A ganglion is a fluid-filled sac that grows from the wrist joint capsule or a tendon sheath. They account for 60–70% of all lumps that appear on the wrist. Completely benign — not cancerous at all — but when they press on nearby structures, they cause a nagging ache on the top of the wrist that worsens when you bend it back.
Some patients notice them literally overnight. Others have had one quietly sitting there for months before it starts causing pain. Either way, it’s worth having assessed rather than guessing.
3. Dorsal Wrist Impingement
This one catches a lot of gym-goers and yoga practitioners off guard. When you extend the wrist under load — think push-ups, front rack barbell position, downward dog — the soft tissue at the back of the joint gets pinched between the carpal bones. Do that repeatedly and you get a very specific, sharp pain on the back of the wrist when bending backwards.
The good news: it responds brilliantly to physio. We address the joint mechanics, build up the surrounding stabilizers, and look at what’s driving the impingement in the first place—usually a technique issue or a mobility restriction.
4. Scapholunate Ligament Injury
This is the one that gets missed most often. The scapholunate ligament connects two small central wrist bones and is critical for joint stability. A fall onto an outstretched hand, or sometimes just prolonged repetitive loading, can strain or tear it. The result is central-back wrist pain, a clicking or clunking sensation under load, and grip weakness.
Here’s the problem: it often looks completely normal on a standard X-ray. You need MRI arthrography to see it properly. I always push for imaging when I suspect a scapholunate injury because leaving it untreated can mean wrist instability and early arthritis down the line—and that’s not a position you want to be in.
5. Carpal Boss
A bony lump at the base of the index or middle finger metacarpal. Hard, fixed, doesn’t move when you press it. Tender with direct pressure and worse with repetitive use. Some patients have lived with one for years before it becomes symptomatic. It’s not harmful, but it can be persistently uncomfortable.
6. ECU Tendinopathy
The extensor carpi ulnaris tendon runs down the back-ulnar side of the wrist — towards the little finger. Overuse from racket sports, rowing, or any repetitive gripping and rotating will inflame it. Produces aching on the outer-back of the wrist with gripping and forearm rotation. Often overlaps with ulnar-sided wrist pain, which is why accurate assessment matters.
7. Desk-Work RSI — The One Nobody Sees Coming
This is probably the most common thing I see in Aylesbury patients. Hours at a keyboard with the wrist slightly extended — not painfully so, just a few degrees — puts the extensor tendons under continuous low-level tension. Week after week. Month after month. Until one Monday the wrist is sore all day and you don’t know why, because nothing specific happened.
That’s the nature of cumulative RSI. There isn’t a moment of injury. The pain just accumulates over time until it crosses a threshold. The fix requires treating the tendons and—just as importantly— sorting out the workstation. Without that second part, it comes back.
How Does Dorsal Wrist Pain Actually Feel?
It varies quite a bit depending on the cause, but here’s what patients typically report:
- A dull ache on the back of the wrist—building with activity and easing with rest. Worse as the day goes on.
- Sharp pain when bending the wrist backwards — during push-ups, planks, yoga, or front rack work at the gym.
- A lump or swelling on the back of the wrist—usually a ganglion cyst or, less commonly, a carpal boss.
- Clicking or clunking with movement — particularly with forearm rotation. This always needs investigation.
- Tenderness on direct pressure — over the back of the wrist bones or between the tendon lines.
- Stiffness first thing in the morning — that loosens up after 10–15 minutes of movement.
- Weakness — dropping things, struggling to open jars, reduced grip under load.
Note-⚠️ Go to A&E if:
Your dorsal wrist pain followed a fall, and you have significant swelling, visible deformity, or you can’t move the wrist. Scaphoid fractures and scapholunate tears regularly appear normal on initial X-rays—don’t assume a clear X-ray means nothing is wrong.
How We Diagnose Dorsal Wrist Pain at Phoenix Physio Aylesbury
Getting this right is everything. A physiotherapy assessment for dorsal wrist pain isn’t just prodding around until something hurts—it’s a structured process of elimination.
In clinic, I work through:
- History — how long has the pain been there, what makes it worse, what you do for work and sport, whether there was any injury
- Palpation — pressing on specific anatomical landmarks to identify exactly which structure is most tender
- Movement testing — both active and passive, to identify which wrist directions reproduce the pain
- Provocative tests — the dorsal impingement test, the scaphoid shift test, the ECU synergy test, and others depending on findings
- Tendon loading — assessing how the tendons respond to progressive load to gauge severity and stage of injury
- Ergonomic and postural review — particularly for patients whose symptoms are driven by their desk setup or work activities
If I suspect a ganglion, scapholunate injury, or carpal boss that needs imaging to confirm, I’ll arrange the appropriate referral—an ultrasound for soft tissue, an X-ray or CT for bony structures, and an MRI arthrography for ligament integrity. No guessing.
Treatment for Dorsal Wrist Pain — What Actually Works
There isn’t a single treatment that works for every type of dorsal wrist pain. What works for impingement won’t work for tendinopathy, and vice versa. Here’s how I approach each:
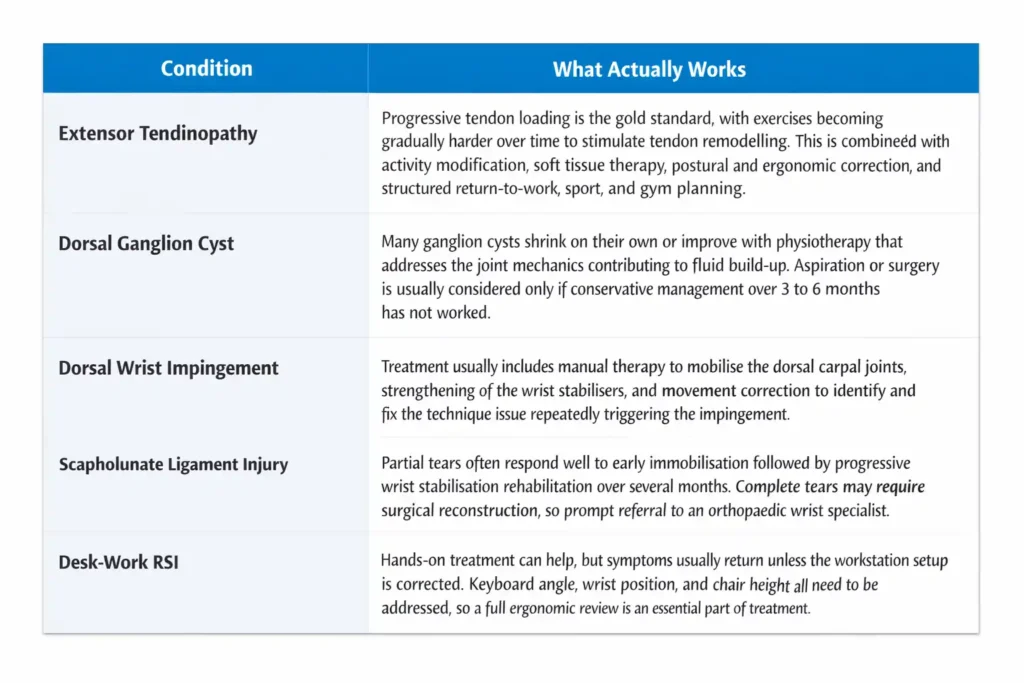
Extensor Tendinopathy
Progressive tendon loading is the gold standard — and by progressive, I mean genuinely progressive. Not the same exercises at the same weight forever. The tendon needs to be systematically challenged to drive the remodelling process. Combined with:
- Activity modification — temporarily reducing the specific repetitive activity that’s driving the irritation
- Soft tissue therapy — manual treatment to reduce pain, restore normal tendon glide and reduce tightness in the forearm
- Postural and ergonomic correction — especially for desk workers
- Return-to-activity planning — structured return to work, sport, and gym once the tendon is ready
Dorsal Ganglion Cyst
Many ganglion cysts shrink on their own, or with physio that addresses the underlying joint mechanics causing the fluid accumulation. I tend not to rush patients toward aspiration or surgery — that’s a second-line option if conservative management over 3–6 months hasn’t worked. A lot of patients are relieved to hear they don’t need a procedure immediately.
Dorsal Wrist Impingement
This type of condition usually needs three things working together:
- Manual therapy to mobilise the dorsal carpal joints and create more space for the soft tissue
- Strengthening the wrist stabilisers so the joint is better supported during loaded extension
- Movement correction — finding and fixing whatever technique issue is repeatedly triggering the impingement
Scapholunate Ligament Injury
Partial tears respond well to conservative management—immobilization early on, then progressive wrist stabilization rehabilitation over several months. Complete tears are a different matter and may need surgical reconstruction. I refer to an orthopedic wrist specialist promptly when I suspect a complete tear. Time matters here.
Desk-Work RSI
Hands-on treatment helps, but it’s not enough on its own. Without fixing the keyboard angle, the wrist position, or the chair height, the symptoms come back. I do a full workstation review as part of treatment for these patients. The ergonomic correction is non-negotiable.
Exercises for Dorsal Wrist Pain — Where to Start
I want to be straightforward about this: these exercises are appropriate for most mild-to-moderate dorsal wrist pain once the acute, inflamed phase has settled. If you’ve just had a sharp pain flare in the last week, hold off and let things calm down first. If you have any doubt about whether these are right for your specific situation—get it assessed.
Exercise 1 — Wrist Flexor Stretch
Arm extended in front of you, elbow straight, palm facing away. Use your other hand to gently pull the fingers back toward your body until you feel a stretch along the back of the forearm and wrist.
Exercise 2 — Prayer Stretch
Both palms together in front of your chest, prayer position. Slowly lower your joined hands down toward your waist, keeping palms pressed, until you feel a stretch across the backs of both wrists.
Exercise 3 — Wrist Extension Strengthening
Forearm resting on a table, palm down, hand hanging freely over the edge. Hold something light — 0.5kg to start. Slowly raise the hand up into extension, hold 2 seconds, lower back down over about 3 seconds. Controlled throughout.
Exercise 4 — Wrist Circles
Elbow supported on a table. Make slow, controlled circles with the wrist — 10 clockwise, 10 anticlockwise. That’s it.
Exercise 5 — Grip Strengthening
Squeeze a soft ball or folded towel as firmly as you comfortably can for 5 seconds. Release fully. Repeat 10 times.
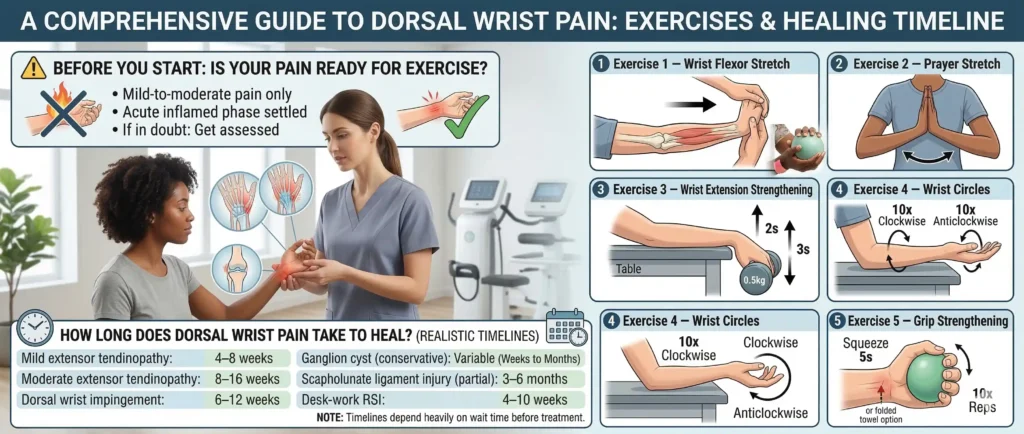
How Long Does Dorsal Wrist Pain Take to Heal?
Honestly? It depends on how long you’ve been waiting before getting it treated. That’s not me trying to guilt you into booking — it’s just the reality. Tendons that have been irritated for two months take longer to fix than tendons that have been irritated for two weeks. The tissue response is different.
Here’s a realistic picture based on what I see clinically:
- Mild extensor tendinopathy: 4–8 weeks with consistent treatment and activity modification
- Moderate extensor tendinopathy: 8–16 weeks — needs a proper progressive loading programme
- Dorsal wrist impingement: 6–12 weeks, less if the triggering activity is modified early
- Ganglion cyst (conservative): Variable — some settle in weeks, others need aspiration
- Scapholunate ligament injury (partial): 3–6 months of rehabilitation
- Desk-work RSI: 4–10 weeks once the ergonomic driver is corrected alongside treatment
Preventing Dorsal Wrist Pain — Practical Advice for Aylesbury Patients
Most of the dorsal wrist pain I treat in Aylesbury is preventable. These are the habits that make the biggest difference:
- Neutral wrist position at the keyboard — wrist straight, not cocked upwards. A wrist rest helps if you’re struggling to maintain this without thinking about it.
- Regular stretching breaks — 60 seconds of wrist flexor stretching every 30 minutes of keyboard time makes a measurable difference to cumulative tendon load. Set a timer if you need to.
- Gradual loading in the gym — this is the one gym-goers ignore most often. Sudden increases in training volume or load are the most common cause of extensor tendinopathy in gym populations. Progress gradually.
- Warm up the wrists before training — wrist circles and a few light loaded extensions before pressing or pulling movements costs you 90 seconds and significantly reduces impingement and tendon injury risk.
- Adjust your yoga or gymnastics wrist position — if you’re getting pain in positions like downward dog or push-up holds, try a slight reduction in wrist extension — use fists or yoga wedges to reduce the range. Your physio can advise on modifications.
Why choose Phoenix Physio Aylesbury for dorsal wrist pain?
Choosing the right physiotherapist for dorsal wrist pain makes the difference between a problem that resolves completely and one that keeps coming back. At Phoenix Physio Aylesbury, we do not treat every wrist the same way. We start with an accurate diagnosis—identifying the exact structure causing your pain before deciding on treatment. That matters because extensor tendinopathy, dorsal wrist impingement, and a scapholunate ligament injury all feel similar but require entirely different approaches.
Our Chartered Physiotherapists, including Tristan Hardy, who holds an MSc in Physiotherapy and brings over 8 years of hands-on MSK experience across both NHS and private practice, treat every patient with the same evidence-based rigor. We do not just treat the wrist—we assess the full picture.
That includes your workstation setup, your training technique, your posture, and whatever repetitive pattern drove the injury in the first place. Without fixing that, the pain comes back. Every time. We offer same-week appointments because wrist pain that has been present for weeks is harder to treat than wrist pain caught early. Serving patients from Aylesbury, Wendover, Thame, Haddenham, and across Buckinghamshire, one session is all it takes to get a clear diagnosis and a plan.
Conclusion
Dorsal wrist pain rarely gets better on its own — but it responds extremely well to the right treatment when caught early. Whether it is overworked tendons, a ganglion cyst, wrist impingement, or desk work quietly taking its toll, the answer is the same: accurate diagnosis first, then treatment that fixes the cause — not just the symptoms.
If your wrist has been painful for more than two weeks, is affecting your work or training, or keeps coming back—that is your sign to come in.
One session. One clear plan. Let’s get your wrist right.
FAQs
What is causing pain on the back of my wrist?
The most common causes are extensor tendinopathy from overuse, a dorsal ganglion cyst, dorsal wrist impingement, or a scapholunate ligament issue. Without an assessment, it’s genuinely difficult to tell which one you have — because the pain location overlaps between causes, but the treatment is different for each.
Why does my wrist hurt when I bend it backwards?
Pain on extension is a hallmark of dorsal wrist impingement or extensor tendinopathy. In impingement, the dorsal capsule is being mechanically pinched. In tendinopathy, the tendons are loaded at the end of range. Either way, avoid forcing the movement—both respond well to physio when caught early.
Is a lump on the back of my wrist serious?
In the vast majority of cases, it’s a dorsal ganglion cyst—benign, fluid-filled, and not cancerous. But any new or growing lump deserves a proper assessment to confirm that’s what it is. Don’t just assume. A physiotherapy assessment can usually identify a ganglion cyst clinically without needing imaging.
Can physiotherapy fix dorsal wrist pain?
For most causes, yes. Extensor tendinopathy, dorsal impingement, and ECU tendinopathy all have strong evidence supporting physiotherapy as first-line treatment. Even ganglion cysts regularly reduce in size when we treat the underlying joint mechanics driving the fluid accumulation.
How long will my dorsal wrist pain take to go away?
Mild cases treated early can resolve in 4–8 weeks. Moderate conditions may take 3–6 months. The single biggest factor in how quickly you recover is whether you address both the symptoms and the underlying cause — the activity or posture driving the injury in the first place.
Do I need a wrist brace for dorsal wrist pain?
Sometimes short-term, yes — particularly if pain is disturbing sleep or you need to keep working during recovery. But a brace is a management tool, not a treatment. Long-term reliance without active rehabilitation creates weakness in the very muscles you need to protect the joint. Use it short-term while you’re doing the rehab work.