Introduction
Frozen shoulder (adhesive capsulitis) is a condition where the tissue capsule surrounding the shoulder joint thickens and scars, progressively limiting all movement across three stages: freezing (acute pain, 6 wks–9 months), frozen (stiffness dominates, 4–12 months), and thawing (gradual recovery, 6 months–2 years). The most effective treatment is early physiotherapy—joint mobilization, progressive stretching, and targeted strengthening—which shortens recovery and prevents permanent stiffness. Without treatment, up to 40% of patients retain long-term limitations.
What is Frozen Shoulder?
Frozen shoulder — medically termed adhesive capsulitis — occurs when the glenohumeral joint capsule (the soft tissue sleeve surrounding your shoulder) becomes chronically inflamed, then thickens and contracts around the ball-and-socket joint. Unlike a rotator cuff tear, where tendons are damaged, frozen shoulder affects the entire capsule. The result is a shoulder that resists movement in every direction — not just when lifted overhead.
The condition affects an estimated 2–5% of the general UK population, with the highest incidence in people aged 40–60. It is not dramatic in its onset — no fall, no pop, no obvious moment of injury. It creeps in over weeks or months, which is exactly why so many people dismiss the early warning signs until the shoulder becomes significantly restricted.
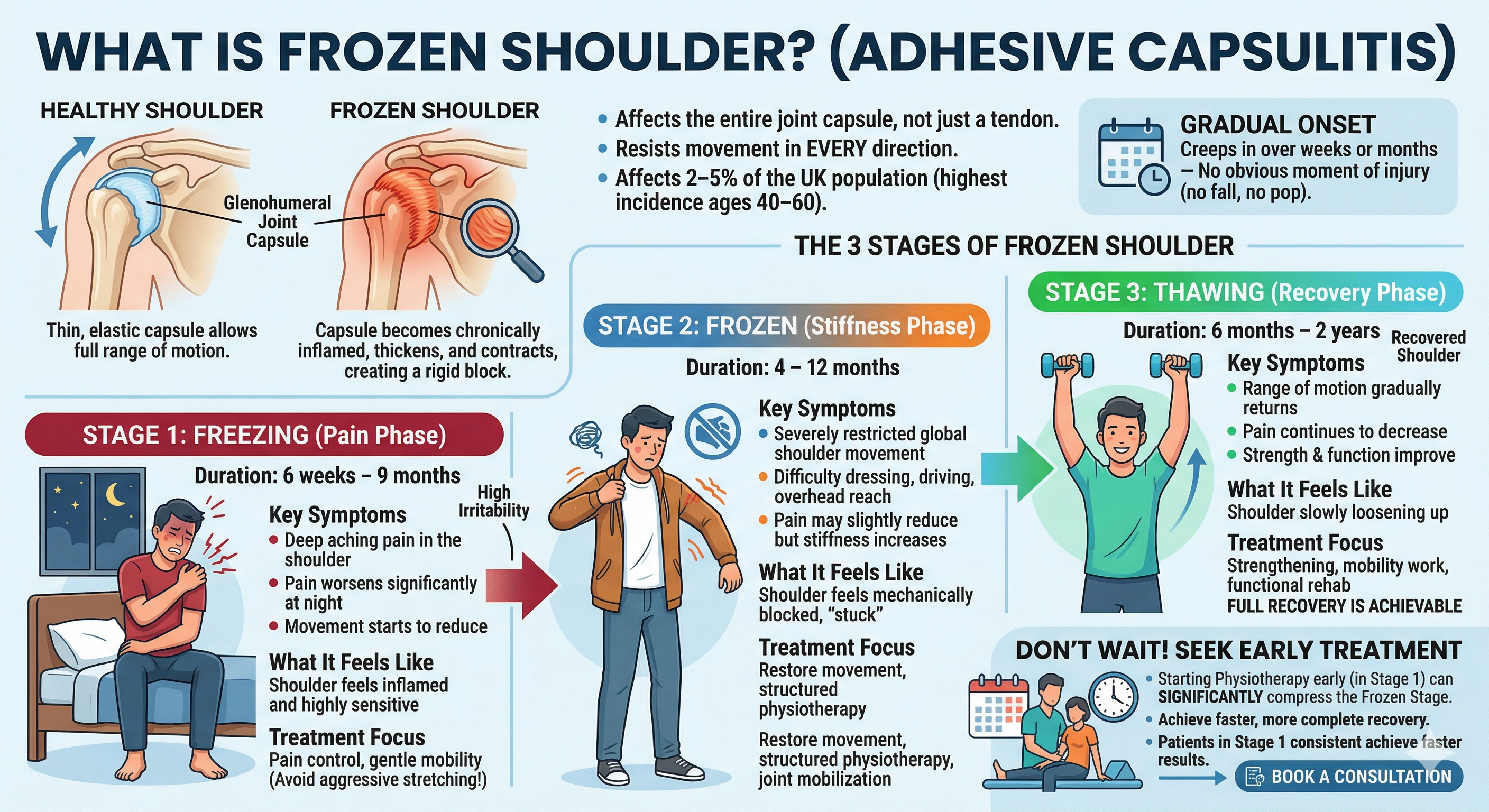
The 3 Stages of Frozen Shoulder
Understanding which stage you are in is the most important thing you can do — because treatment strategy shifts significantly between stages. Many patients arrive at our Wendover clinic already in the frozen stage, having waited out several months of worsening pain.
Stage 1
- Deep, aching pain in the shoulder
- Pain worsens at night — often severe enough to wake you
- Movement starts to reduce, especially external rotation
- Shoulder is highly irritable; even small movements hurt
Stage 2
- Pain may reduce slightly compared to Stage 1
- Severe, global restriction of all shoulder movements
- Dressing, driving, and reaching overhead become difficult
- Joint feels mechanically blocked, not just painful
Stage 3
- Range of motion gradually returns
- Pain continues to decrease
- Strength and function improve with consistent physiotherapy
- Full recovery is achievable—though timing varies
| Stage | Phase Name | Duration | Pain Level | Mobility | Key Symptoms | What It Feels Like | Treatment Focus |
|---|---|---|---|---|---|---|---|
| Stage 1 | Freezing (Pain Phase) | 6 weeks – 9 months | High, worsening (especially at night) | Gradually reducing | Deep aching pain, sharp pain with movement, disturbed sleep | Shoulder feels inflamed and sensitive | Pain control, gentle mobility, avoid aggressive stretching |
| Stage 2 | Frozen (Stiffness Phase) | 4 – 12 months | Moderate (less than Stage 1) | Severely restricted | Stiffness, difficulty dressing, driving, overhead reach | Shoulder feels “stuck” or blocked | Restore movement, structured physio, joint mobilization |
| Stage 3 | Thawing (Recovery Phase) | 6 months – 2 years | Low, improving | Gradually returning | Improved range, reduced pain, better function | Shoulder slowly loosening up | Strengthening, mobility work, functional rehab |
Don’t wait for Stage 3 to seek treatment. The freezing stage is the optimal intervention window. Starting physiotherapy early can compress the frozen stage significantly, sometimes preventing it from reaching its worst potential duration. Patients who begin treatment in Stage 1 consistently achieve faster, more complete recovery.
Causes of Frozen Shoulder
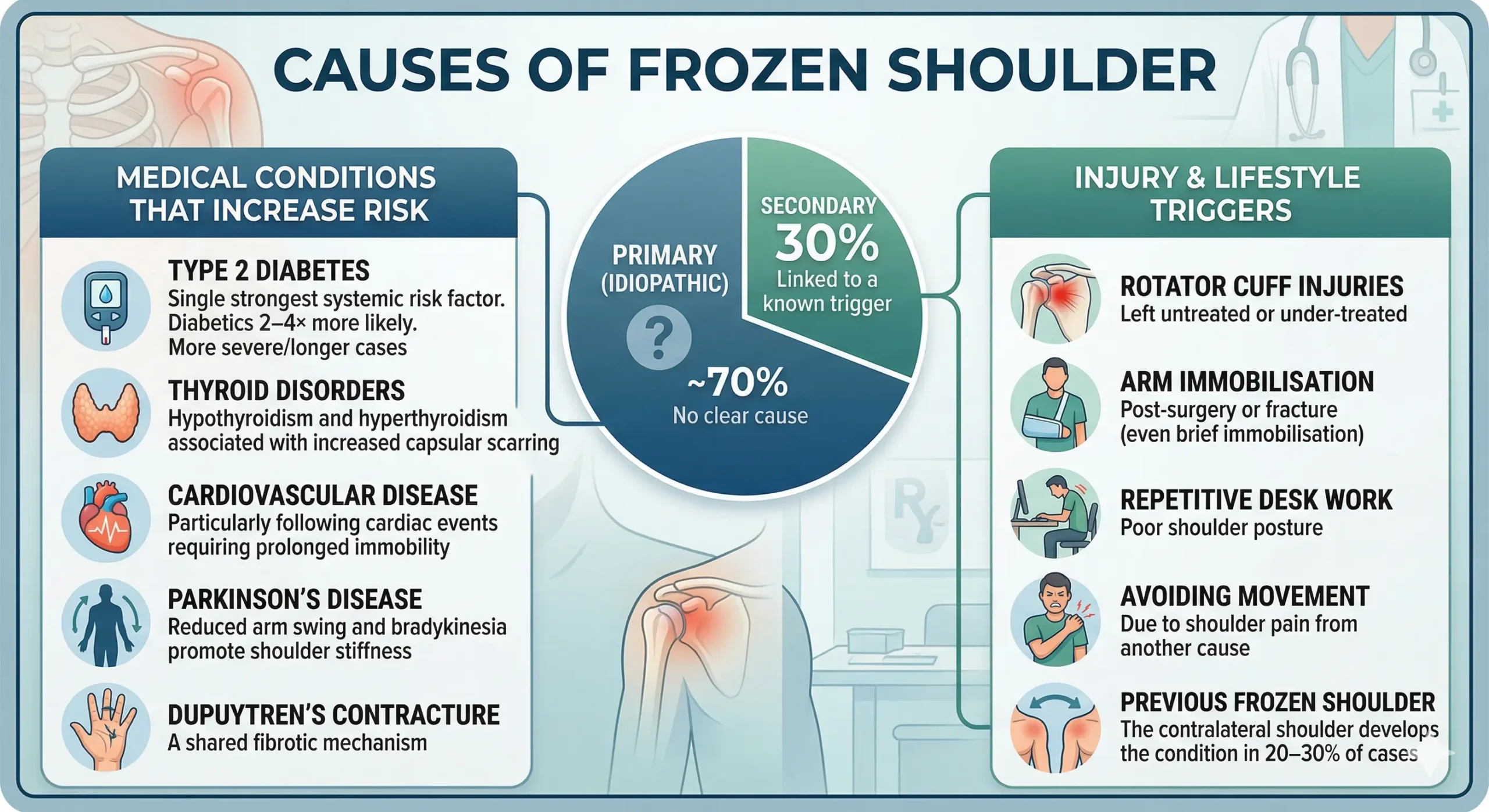
Frozen shoulder is classified as either primary (idiopathic — no clear cause) or secondary (linked to a known trigger). Primary cases account for roughly 70% of presentations. The remaining 30% are associated with identifiable risk factors:
Medical Conditions That Increase Risk
- Type 2 Diabetes — the single strongest systemic risk factor. Diabetics are 2–4× more likely to develop frozen shoulder and often experience more severe, longer-lasting cases
- Thyroid disorders — both hypothyroidism and hyperthyroidism are associated with increased capsular scarring
- Cardiovascular disease — particularly following cardiac events requiring prolonged immobility
- Parkinson’s disease—reduced arm swing and bradykinesia promote shoulder stiffness
- Dupuytren’s contracture — a shared fibrotic mechanism
Injury & Lifestyle Triggers
- Rotator cuff injuries left untreated or under-treated
- Arm immobilisation post-surgery or fracture (even brief immobilisation can trigger onset)
- Repetitive desk work with poor shoulder posture
- Avoiding movement due to shoulder pain from another cause
- Previous frozen shoulder — the contralateral shoulder develops the condition in 20–30% of cases
Symptoms of Frozen Shoulder
The hallmark of frozen shoulder is progressive loss of range of motion in all directions. This is the key distinction from other shoulder conditions where only certain movements are restricted. If your shoulder hurts when you lift forward but moves freely sideways, that is likely a different diagnosis.
Symptoms That Should Prompt a Physio Assessment
- Shoulder pain lasting more than 3 weeks without a clear injury
- Night pain severe enough to wake you or prevent comfortable sleep
- Difficulty getting your arm behind your back (clasping a bra, tucking a shirt)
- Difficulty lifting your arm past shoulder height
- A gradual sense that the shoulder is “seizing up” rather than a sudden injury
- Stiffness that is progressively worsening, not improving
How Is Frozen Shoulder Diagnosed?
Frozen shoulder is primarily a clinical diagnosis—meaning it is identified through assessment, not imaging alone. At Phoenix Physio, our chartered physiotherapists perform a structured evaluation that includes:
Physical Assessment
We measure active range of motion (how far you can move the arm yourself) and passive range of motion (how far the physiotherapist can move it for you). In frozen shoulder, both are significantly restricted — this is the distinguishing clinical sign. Shoulder impingement and rotator cuff tears typically preserve passive movement.
Imaging
X-rays are used to rule out bony pathology such as arthritis or calcific tendinopathy. An MRI scan is indicated when the diagnosis is uncertain, or when a concurrent rotator cuff tear needs to be excluded. MRI may show a thickened capsule and reduced capsular volume in frozen shoulder, though imaging is not always necessary to begin treatment.
Frozen shoulder is primarily a clinical diagnosis-.
Our physiotherapists can assess your shoulder at our Chilterns Neuro Centre clinic (HP22 5LX). No GP referral is needed. An initial 45-minute assessment— during which you will receive a diagnosis, an explanation of your stage, and a personalized treatment plan.
Frozen Shoulder Treatment: What Actually Works in 2026
The good news: frozen shoulder is fully treatable. The strategy changes depending on which stage you are in, but physiotherapy remains the backbone of evidence-based management across all three stages.
1. Physiotherapy — The Gold Standard
Physiotherapy for frozen shoulder encompasses several techniques that our Wendover physio team integrates into a single, coherent treatment plan:
- Joint mobilisation — hands-on techniques to gradually stretch the contracted capsule, restore glide, and decompress the joint. Particularly effective in the frozen and early thawing stages
- Progressive stretching — structured daily stretching targeting external rotation, abduction, and internal rotation — the three movements most restricted by adhesive capsulitis
- Soft tissue release — addressing secondary muscle tightness in the pectorals, subscapularis, and posterior capsule that develops as the shoulder locks down
- Strengthening — progressive rotator cuff and scapular stabiliser exercises introduced in the thawing stage to restore full functional strength
- Postural correction — addressing the thoracic stiffness and scapular dysfunction that often accompany prolonged shoulder restriction
2. Corticosteroid Injections
Ultrasound-guided steroid injections into the glenohumeral joint reduce acute inflammation and provide meaningful short-term pain relief, especially in the freezing stage. Evidence supports their use as an adjunct to physiotherapy — not a standalone treatment. Patients who receive an injection followed by structured physiotherapy achieve better outcomes than those who receive either alone.
3. Hydrodilatation (Distension Arthrography)
A more advanced injection procedure where sterile fluid is injected into the joint capsule under pressure, physically stretching the contracted capsule. Recommended when standard injections and physiotherapy have not produced sufficient improvement after 3–6 months. Available via GP or consultant referral.
4. Surgery — A Last Resort
Arthroscopic capsular release and manipulation under anaesthesia (MUA) are reserved for refractory cases — typically when 12–18 months of conservative management has failed to restore adequate function. Fewer than 10% of frozen shoulder cases ultimately require surgical intervention
Best Exercises for Frozen Shoulder
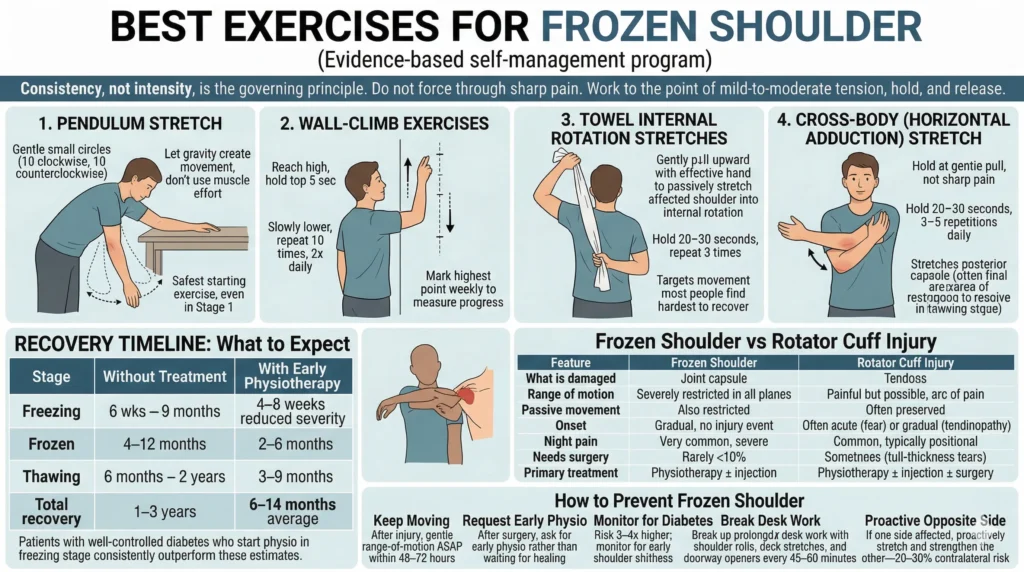
These exercises form the evidence-based self-management program we give all frozen shoulder patients at Phoenix Physio. Consistency, not intensity, is the governing principle. Do not force through sharp pain. Work to the point of mild-to-moderate tension, hold, and release.
1 Pendulum Stretch
Stand beside a table and lean forward with your good arm supporting you. Let the affected arm hang freely. Gently swing it in small circles—10 clockwise, 10 counterclockwise. Let gravity create the movement; don’t use muscle effort. Gradually increase the diameter of circles as weeks pass. This is your safest starting exercise even in Stage 1.
2 Wall-Climb Exercises
Stand facing a wall and walk your fingers up the surface, reaching as high as you can without shrugging. Hold the top position for 5 seconds. Slowly lower. Repeat 10 times, twice daily. Mark your highest point weekly—this is your most visible measure of progress in the thawing stage.
3 Towel Internal Rotation Stretches
Hold a towel behind your back—dominant hand at the top, affected hand at the bottom. With the effective hand, gently pull upward to passively stretch the affected shoulder into internal rotation. Hold 20–30 seconds. Repeat 3 times. This exercise targets the movement that most people find hardest to recover from when they have a frozen shoulder.
4 Cross-Body (Horizontal Adduction) Stretch
Use your good arm to lift the affected elbow and draw the arm across your chest, holding at the point of gentle pull—not sharp pain. Hold 20–30 seconds. Do 3–5 repetitions daily. This stretches the posterior capsule, which often becomes the final area of restriction to resolve in the thawing stage.
Recovery Timeline: What to Expect
The most common question we hear at Phoenix Physio Wendover is: “How long will this take?” The answer depends on when you start treatment, your overall health, and how consistently you follow your home exercise programme.
| Stage | Without Treatment | With Early Physiotherapy |
|---|---|---|
| Freezing | 6 weeks – 9 months | 4–8 weeks (reduced severity) |
| Frozen | 4–12 months | 2–6 months |
| Thawing | 6 months – 2 years | 3–9 months |
| Total recovery | 1–3 years | 6–14 months (average) |
These timelines are averages. Patients with well-controlled diabetes, who start physio in the freezing stage and maintain daily home exercises, consistently outperform these estimates. Patients who begin treatment in the frozen stage can still achieve full recovery, but the rehabilitation arc is longer.
Frozen Shoulder vs Rotator Cuff Injury
These two conditions are frequently confused — both cause shoulder pain and weakness, and both respond to physiotherapy. However, the underlying anatomy, movement pattern, and treatment approach differ significantly.
| Feature | Frozen Shoulder | Rotator Cuff Injury |
|---|---|---|
| What is damaged | Joint capsule | Tendons (supraspinatus, infraspinatus, subscapularis) |
| Range of motion | Severely restricted in all planes | Painful but possible; arc of pain |
| Passive movement | Also restricted | Often preserved |
| Onset | Gradual, no injury event | Often acute (tear) or gradual (tendinopathy) |
| Night pain | Very common, severe | Common, typically positional |
| Needs surgery | Rarely (<10%) | Sometimes (full-thickness tears) |
| Primary treatment | Physiotherapy ± injection | Physiotherapy ± injection ± surger |
How to Prevent Frozen Shoulder
While primary frozen shoulder can occur without a clear trigger, secondary cases are largely preventable. The key principle is to keep the shoulder moving. Any period of prolonged immobility — whether from injury, surgery, or occupational posture — is an opportunity for the capsule to begin to scar.
- After any shoulder injury, begin gentle range-of-motion exercises within pain tolerance as soon as possible—even within 48–72 hours in many cases
- If recovering from shoulder or upper limb surgery, request early physiotherapy rather than waiting for “enough healing time.”
- If you have type 2 diabetes, monitor for early shoulder stiffness—your risk is 3–4× higher and early intervention is critical
- Break up prolonged desk work with shoulder rolls, neck stretches, and doorway chest-opener stretches every 45–60 minutes
- If you had frozen shoulder on one side, proactively stretch and strengthen the other—contralateral risk is 20–30%
Why Choose Phoenix Physio for Frozen Shoulder Treatment?
Our chartered physiotherapists combine clinical expertise with a practical, results-driven approach to recovery. You’re not put on a generic pathway—everything is built around your condition, your stage, and how your body responds to treatment.
Charlotte Gailor (BSc, St George’s London, 2014) and Tristan Hardy (MSc Physiotherapy, BSc Sport Science) specialise in musculoskeletal and orthopaedic conditions
No GP referral needed: Book directly and be seen within days, not months
Personalised treatment plans: No one-size-fits-all protocols—your plan is tailored to your lifestyle and goals
Home exercise support: You’ll receive a structured programme by email after every session to keep progressing between appointments
Conclusion: Frozen Shoulder Recovery Starts With Action
Frozen shoulder is slow, frustrating, and often misunderstood—but it’s completely manageable when you approach it the right way. The biggest mistake is waiting. By the time most people seek help, they’ve already moved from the painful freezing stage into full stiffness, which means longer recovery.
Here’s the reality:
- Early intervention shortens recovery
- The right treatment depends on your stage
- Consistency with physiotherapy is what restores movement
Ignore it, and you’re looking at 1–3 years of limitation. Act early, stay consistent, and most people regain strong, functional movement much sooner.
If your shoulder pain has lasted more than a few weeks or your mobility is dropping, don’t guess—get it assessed. The sooner you start, the easier it is to reverse.
Frequently Asked Questions About Frozen Shoulder
What is the fastest way to cure a frozen shoulder?
There is no overnight cure, but early physiotherapy is the single most effective intervention. A combination of joint mobilisation, targeted stretching, and guided exercises — started during the freezing stage — significantly shortens overall recovery. Corticosteroid injections can reduce inflammation short-term, but physiotherapy addresses the underlying capsular restriction. Patients who begin treatment early and maintain daily home exercises achieve the best outcomes.
How long does frozen shoulder last?
Without treatment, frozen shoulder typically lasts 1–3 years across its three stages. With consistent physiotherapy started early, most patients achieve meaningful functional recovery within 6–12 months. The freezing stage lasts 6 weeks to 9 months, the frozen stage 4–12 months, and the thawing stage 6 months to 2 years. Duration varies based on age, health conditions (especially diabetes), and how early treatment is started.
Can a physiotherapist fix a frozen shoulder without surgery?
In the vast majority of cases, yes. Fewer than 10% of frozen shoulder patients ultimately require surgery. Physiotherapy — specifically joint mobilisation, progressive stretching, and staged strengthening — is the evidence-based first-line treatment and produces full recovery in most patients. Surgery (arthroscopic capsular release or manipulation under anaesthesia) is reserved for cases where 12–18 months of conservative management has not achieved adequate function.
Is frozen shoulder the same as a rotator cuff tear?
No — these are distinct conditions. Frozen shoulder involves tightening of the entire joint capsule, restricting movement in all planes. A rotator cuff tear involves tendon damage, and movement is painful but typically still possible. A physiotherapist can distinguish the two through clinical assessment (particularly by testing passive range of motion). MRI provides confirmation when needed.
Should I use heat or ice for frozen shoulder pain?
Both have a role. Apply heat (warm compress or shower) for 5–10 minutes before stretching or exercise — this relaxes the capsule and improves tissue extensibility. Apply ice after exercise or during acute pain flares to reduce inflammation. Neither option replaces physiotherapy, but when used correctly alongside your exercise program, both can meaningfully improve your comfort between sessions.
When should I see a physiotherapist for shoulder pain?
Do not wait until your shoulder is fully locked. See a physiotherapist if you have: shoulder pain lasting more than 2–3 weeks without improvement; difficulty lifting your arm above shoulder height; night pain disturbing your sleep; or stiffness that is getting progressively worse rather than better. Early assessment means earlier diagnosis, earlier treatment, and a significantly shorter recovery.