Introduction
Shoulder pain rarely shows up without a reason—and in the UK, the rotator cuff is behind most of it. If lifting your arm hurts, your shoulder clicks, or the pain wakes you at night, this isn’t something to ignore. It’s a clear sign that the rotator cuff isn’t coping with the load you’re putting through it.
In Aylesbury and across Buckinghamshire, we see this pattern every day. What starts as a mild ache from gym training, desk posture, or repetitive work quickly turns into persistent pain, weakness, and restricted movement. The longer it’s left, the harder it becomes to fix.
This guide breaks it down properly—what the rotator cuff actually is, why it gets injured, how to recognise the symptoms early, and most importantly, how to recover with the right physiotherapy approach. No fluff, no generic advice—just what works.
What is the Rotator Cuff?
Your shoulder is one of the most mobile joints in the entire body. That freedom of movement — being able to reach behind your back, throw a ball, or lift a box onto a shelf — is made possible by the rotator cuff.
Put simply, the rotator cuff is a group of four muscles and their attached tendons. Together, they form a sleeve around the head of your upper arm bone (the humerus) and hold it firmly inside the shallow socket of the shoulder blade (the glenoid). Without this muscular cuff, your shoulder would dislocate every time you lifted a cup of tea.
The term “cuff” is actually quite accurate. Imagine pulling on a shirt cuff — it wraps around and secures. The rotator cuff does the same thing to the ball of your shoulder joint. Every time you raise, lower, rotate or stabilise your arm, these muscles are working together in a finely tuned sequence.
When something goes wrong with any part of that system — whether it’s a sudden tear, gradual wear, or irritated tendon — the result is rotator cuff pain. And it can stop you in your tracks.
📍 Local Fact — Aylesbury
Rotator cuff injuries are among the most common shoulder complaints we see at Phoenix Physio in Aylesbury. Whether you’ve been gardening in Buckinghamshire’s countryside, playing tennis at a local club, or simply overdone it at the gym — the rotator cuff is often behind that nagging shoulder pain.
The Four Rotator Cuff Muscles
Understanding which muscles make up your rotator cuff helps you make sense of where pain comes from — and why certain movements hurt more than others.
All four work together as a team. When one is weakened, torn, or inflamed, the others compensate — often leading to a cascade of shoulder problems if left untreated.

What Causes a Rotator Cuff Injury?
Rotator cuff injuries don’t always happen dramatically. In fact, most of the people who walk into our Aylesbury clinic didn’t “do” anything specific. The injury built up quietly over months or years.
Degenerative (Wear and Tear)
This is the most common cause. As we age, the blood supply to tendons decreases. Over time, the tendons become less elastic, more prone to small tears that don’t fully repair themselves. By the time many people feel pain, the degeneration has been going on for years. Repetitive overhead movements at work — painters, plasterers, warehouse staff—accelerate this process considerably.
Acute Traumatic Injury
A fall onto an outstretched arm, a heavy lift that goes wrong, a sudden awkward movement reaching for something in the back seat of a car — these can cause an immediate rotator cuff tear. Younger patients more commonly experience acute injuries, while older patients tend towards degenerative ones.
Shoulder Impingement
Shoulder impingement is closely related to rotator cuff problems. It occurs when the supraspinatus tendon is repeatedly pinched between the top of the arm bone and the roof of the shoulder (the acromion). This friction gradually damages the tendon and, if untreated, can lead to a rotator cuff tear.
Sports-Related Causes
Swimming, cricket, tennis, golf, and throwing sports all demand repetitive overhead shoulder movement. This is why rotator cuff injuries are common sports injuries in Buckinghamshire’s active community — whether at Aylesbury Vale leisure centres, local cricket clubs, or weekend rugby. Poor technique or a sudden increase in training load are common triggers.
Risk Factors
You’re at higher risk if you’re over 40, work in a job involving overhead movements, play racket or throwing sports, smoke (which reduces tendon blood supply), or have a history of shoulder problems. Being male slightly increases your risk, though women are by no means immune.
Symptoms of a Rotator Cuff Injury
Rotator cuff pain has a distinctive character. It often catches people off guard because it can be so persistent—especially at night.
- A dull, deep ache in the shoulder, often felt at the front or side
- Pain when lifting the arm — especially between 60° and 120° of elevation (the “painful arc”)
- Difficulty reaching behind your back — fastening a bra, tucking in a shirt
- Night pain that wakes you from sleep, especially when lying on the affected side
- Weakness when lifting, reaching overhead, or carrying shopping
- A clicking, creaking, or crackling sensation during shoulder movement
- Pain that radiates down into the outer arm (not usually past the elbow)
| Symptom | What It Feels Like | What It Indicates |
|---|---|---|
| Dull shoulder ache | Deep, persistent pain at the front or side of the shoulder | Early rotator cuff irritation or tendinopathy |
| Painful arc (60°–120°) | Sharp pain when lifting the arm sideways | Rotator cuff impingement |
| Difficulty reaching behind back | Struggle with dressing (bra, shirt, belt) | Reduced mobility + tendon involvement |
| Night pain | Pain when lying on the shoulder, disturbed sleep | Bursa inflammation + rotator cuff irritation |
| Weakness in arm | Difficulty lifting, reaching, or carrying weight | Possible tendon tear or muscle dysfunction |
| Clicking or grinding | Cracking, creaking sensation during movement | Joint instability or tendon friction |
| Pain radiating down arm | Discomfort spreading into the upper arm (not past elbow) | Typical rotator cuff referral pattern |
What Does a Rotator Cuff Injury Feel Like vs. a Torn Rotator Cuff?
A rotator cuff strain or tendinopathy produces a persistent ache that worsens with activity. A rotator cuff tear often involves more pronounced weakness. You might find it very difficult — or impossible — to lift your arm past a certain point. A full-thickness tear (where the tendon is completely severed) can result in sudden, dramatic weakness alongside the pain.
Types of Rotator Cuff Injury
Not all rotator cuff injuries are the same. The severity ranges enormously — and this matters for how they’re treated.
Rotator Cuff Tendinopathy
The mildest form. The tendons are irritated and degenerate slightly but remain intact. Pain tends to be worse with specific movements rather than constant. This is the most responsive to physiotherapy and targeted rotator cuff exercises — most people make a full recovery.
Rotator Cuff Calcification
Calcium deposits form within the tendon (usually the supraspinatus). This causes sharp, severe pain that can come on suddenly and be surprisingly intense. Calcific tendinopathy can be extremely painful during the “resorptive” phase — when the calcium deposit begins to break down. Most cases resolve with physiotherapy, though ultrasound-guided needling or surgery is occasionally needed.
Partial Rotator Cuff Tear
Part of the tendon is damaged but the tear doesn’t go all the way through. These are graded by depth. Symptoms are similar to tendinopathy but often more severe. Many partial tears heal well with conservative management — physio, strengthening exercises, and time.
Full-Thickness (Complete) Rotator Cuff Tear
The tendon is completely torn from the bone. Symptoms include significant weakness, often an inability to lift the arm actively. However — perhaps surprisingly—some people with full-thickness tears have minimal pain and function reasonably well. Not every complete tear requires surgery, particularly in older, less active patients.
Massive Rotator Cuff Tear
A tear involving two or more of the four tendons. These are more complex to manage and often require surgical discussion, though results are variable.
How is a Rotator Cuff Injury Diagnosed?
A good diagnosis starts with a thorough clinical assessment. At Phoenix Physio in Aylesbury, we use a structured approach that combines your history, hands-on examination, and, where necessary, imaging.
Clinical Tests
Several special tests help identify which part of the rotator cuff is involved:
- Painful Arc Test — pain between 60°–120° of arm elevation suggests supraspinatus involvement
- Drop Arm Test — inability to hold the arm at 90° indicates a significant supraspinatus tear
- External Rotation Resistance Test — weakness suggests infraspinatus or teres minor involvement
- Belly Press / Lift-Off Test — assesses the subscapularis
- Neer’s & Hawkins-Kennedy Tests — screen for shoulder impingement.
Rotator Cuff Injury Test at Home
🔍 Imaging: MRI and Ultrasound
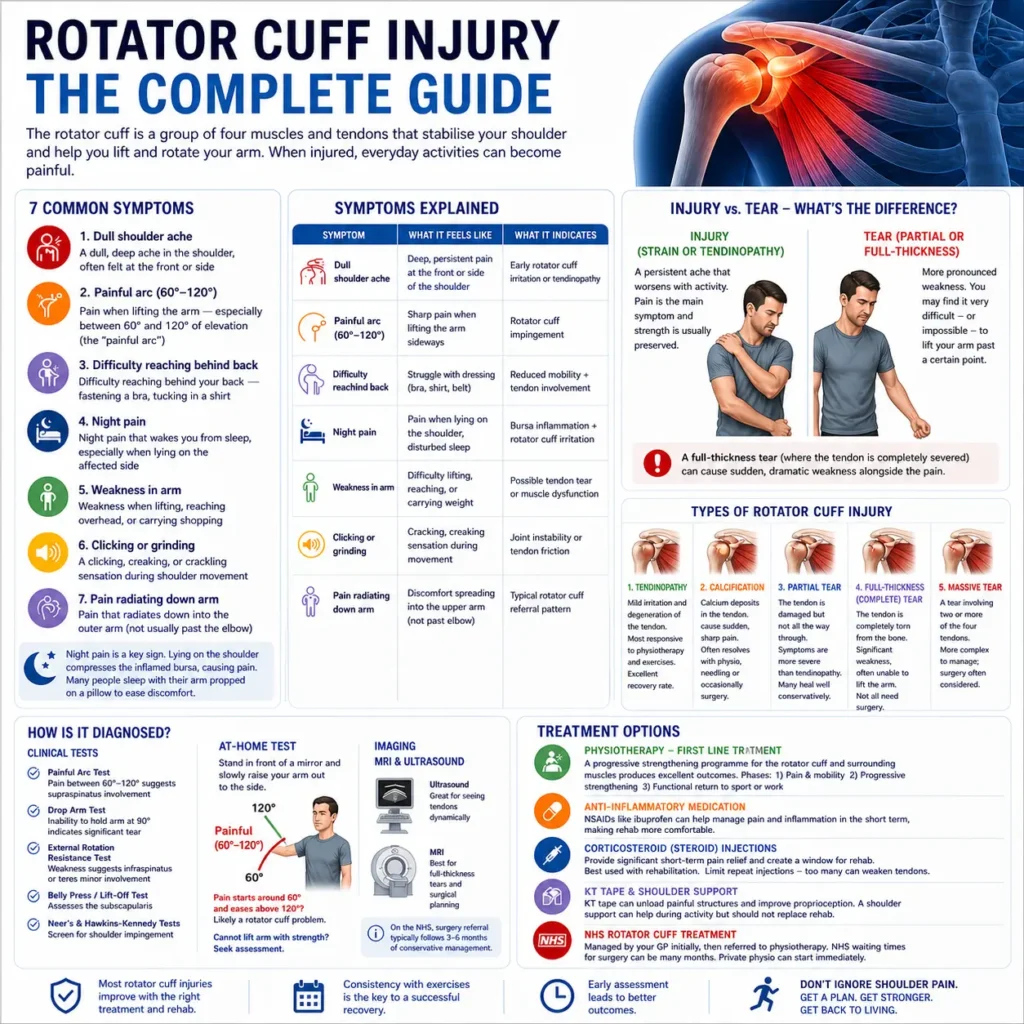
If your GP or physiotherapist suspects a significant tear, you may be referred for an ultrasound or MRI scan. Ultrasound is excellent for assessing tendons dynamically. MRI gives the clearest picture of full-thickness tears and is more useful before surgical planning. On the NHS, rotator cuff surgery referral typically follows a period of at least 3–6 months of conservative management.
Treatment Options — NHS and Private Physio
The good news? The vast majority of rotator cuff injuries respond well to non-surgical treatment. Surgery is reserved for cases where conservative management genuinely hasn’t worked, or where the injury severity demands it from the outset.
Physiotherapy — The First Line of Treatment
This is where the evidence is clearest. Physiotherapy — specifically a progressive strengthening programme for the rotator cuff and surrounding shoulder muscles — consistently produces excellent outcomes. A physiotherapist will assess the specific muscles and movement patterns involved, then design a rehabilitation programme tailored to you.
At Phoenix Physio in Aylesbury, we typically progress rotator cuff rehabilitation through three phases: pain management and gentle mobility, then progressive strengthening, then functional return to sport or work.
Anti-Inflammatory Medication
NSAIDs such as ibuprofen can help manage pain and inflammation in the short term, particularly with acute presentations. They’re not a long-term solution, but used alongside physiotherapy they can make rehabilitation more comfortable. Always follow your GP’s guidance.
Corticosteroid (Steroid) Injections
A cortisone shot into the subacromial space can provide significant short-term pain relief — creating a window in which physiotherapy can be much more productive. They work best when combined with rehabilitation rather than used in isolation. Repeat injections should be limited, as too many can weaken tendon tissue over time.
KT Tape and Shoulder Support
Kinesiology tape (KT tape) applied around the rotator cuff can temporarily unload the painful structures and improve proprioception. A shoulder support or brace for rotator cuff injury can help during activity, though it shouldn’t replace rehabilitation. These are tools to support recovery, not substitutes for it.
NHS Rotator Cuff Treatment
On the NHS, most rotator cuff injuries are managed by your GP initially, then referred to physiotherapy. NHS waiting times for rotator cuff surgery can be significant, often many months. Private physiotherapy in Aylesbury (such as at Phoenix Physio) can begin immediately, meaning you start your recovery without delay.
Best Rotator Cuff Exercises
Exercise is the cornerstone of rotator cuff rehabilitation. These movements rebuild the strength and neuromuscular control the shoulder needs. Start gently — if an exercise produces sharp pain, stop and reassess with your physiotherapist.
- Pendulum SwingsStand and lean forward, letting your affected arm hang loosely. Gently swing it in small circles — 10 clockwise, 10 anticlockwise. This decompresses the shoulder joint and reduces pain and stiffness. Perfect as a first morning exercise
- Isometric External RotationStand side-on to a wall, elbow bent at 90°. Press the back of your hand gently into the wall without moving. Hold for 5 seconds, and repeat 10 times. This activates the infraspinatus and teres minor without loading the painful arc — ideal in the early stages.
- Theraband External RotationFix a resistance band to a door handle. With your elbow at 90°, rotate your forearm outward against the band’s resistance. 3 sets of 15 reps. One of the most evidence-backed rotator cuff strengthening exercises available
- Scapular RetractionSit or stand tall. Gently squeeze your shoulder blades together as if trying to hold a pencil between them. Hold 5 seconds. Repeat 15 times. This re-establishes proper scapular positioning — critical because poor posture is a key driver of shoulder impingement.
- Side-Lying External Rotation (Dumbbell)Lie on your unaffected side. Bend your top elbow to 90°, with a light dumbbell in hand. Slowly rotate your forearm upward. 3 sets of 12 reps. This isolated rotator cuff dumbbell exercise is excellent for building infraspinatus strength without shoulder impingement risk
- Prone Y–T–W RaisesLie face down on a bench. Raise both arms into a Y shape (thumbs up), then T (arms out), then W (elbows bent, hands up). Light dumbbells optional. This targets the lower trapezius and rotator cuff together—addressing the full kinetic chain of the shoulder.
Exercises to Avoid with a Rotator Cuff Injury
Certain movements repeatedly stress the already-damaged tissues and delay recovery. These are the ones to sidestep during rehabilitation:
- Overhead pressing (military press, shoulder press machine) — compresses the supraspinatus tendon against the acromion
- Upright rows — a particularly aggressive movement for shoulder impingement
- Behind-the-neck pull-downs or presses — places the shoulder in a vulnerable impingement position
- Heavy bench pressing — loads the subscapularis under high compressive force
- Dips — places significant strain on the anterior shoulder capsule and subscapularis
- Throwing or serving overhead until fully rehabilitated
The rule of thumb is simple: if the movement causes a sharp pinch at the top of your shoulder, or reproduces your exact pain pattern — stop. Pain is your body’s communication system. Learn to listen to it during rehab.
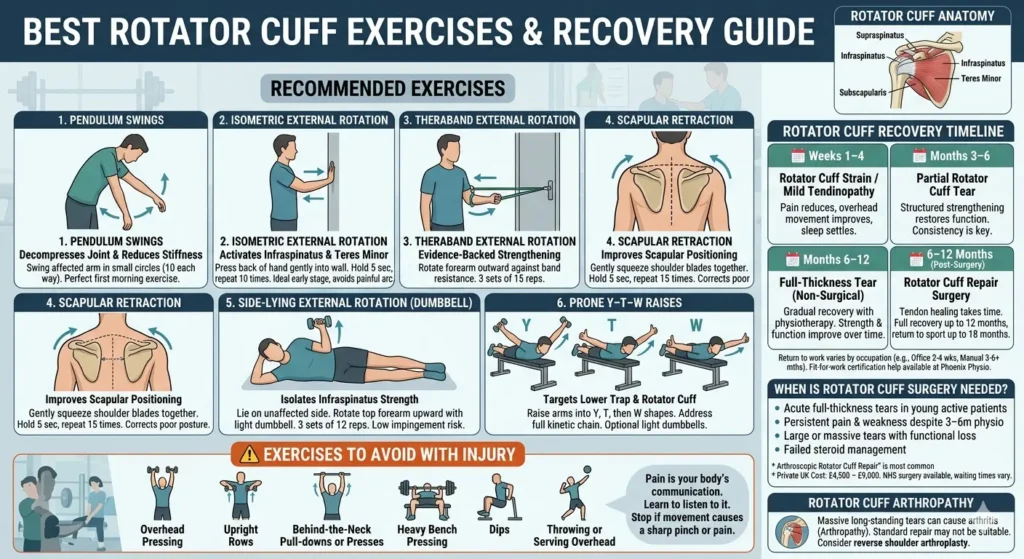
Rotator Cuff Recovery Timeline
| ⏱️ Timeline | 💪 Injury Type | 📈 Recovery Expectation |
|---|---|---|
| 🗓️ Weeks 1–4 | Rotator Cuff Strain / Mild Tendinopathy | Pain reduces with physiotherapy and load management. Overhead movement improves. Sleep disturbance starts to settle. |
| 🗓️ Months 3–6 | Partial Rotator Cuff Tear | Structured strengthening restores function in most cases. Progress depends heavily on exercise consistency and correct rehab progression. |
| 🗓️ Months 6–12 | Full-Thickness Tear (Non-Surgical) | Gradual recovery with physiotherapy. Strength and function improve over time, especially in lower-demand individuals. |
| 🗓️ 6–12 Months (Post-Surgery) | Rotator Cuff Repair Surgery | Tendon healing takes time. Full recovery typically takes up to 12 months, with return to sport sometimes extending to 18 months. |
Rotator cuff injury recovery time off work varies by occupation. Office-based workers may return in 2–4 weeks. Manual workers, those doing overhead tasks, or those post-surgery may need 3–6 months or longer. Fit-for-work certification and phased return planning is something we can help with at Phoenix Physio.
When is Rotator Cuff Surgery Needed?
Surgery is not the first answer for a rotator cuff injury, but for some patients, it becomes the right answer when everything else has been genuinely tried.
Rotator Cuff Repair (Arthroscopic)
The most common surgical procedure is an arthroscopic rotator cuff repair—keyhole surgery performed under general anesthesia. The surgeon reattaches the torn tendon to the bone using small anchors. It’s a technically demanding procedure with generally good results when the right patient is selected.
Who Needs Rotator Cuff Surgery?
- Acute full-thickness tears in younger, active patients — especially if treated within weeks of injury
- Persistent pain and weakness despite a genuine 3–6 month course of physiotherapy
- Large or massive tears causing significant functional loss in active individuals
- Failed steroid injection management
Rotator Cuff Surgery Cost (Private UK)
Private rotator cuff repair surgery in the UK typically costs between £4,500 and £9,000 depending on the hospital, surgeon, and complexity. NHS rotator cuff surgery is available for appropriate cases but NHS waiting times can be considerable. Private physiotherapy post-operatively is essential regardless of how the surgery is funded.
Rotator Cuff Arthropathy
In long-standing, massive rotator cuff tears, the shoulder joint can develop secondary arthritis — a condition called rotator cuff arthropathy. When this is present, a standard rotator cuff repair may no longer be suitable, and a specialist type of shoulder replacement (reverse shoulder arthroplasty) may be considered instead.
When Should You Visit Phoenix Physio Aylesbury?
Here’s the honest answer: sooner than you think.
Many people in Aylesbury and across Buckinghamshire spend weeks — sometimes months — waiting for shoulder pain to resolve on its own. Sometimes it does. Often, it doesn’t. And when it doesn’t, the longer it goes on, the harder it is to shift.
See a physiotherapist promptly if:
- Your shoulder pain has lasted more than two weeks without improving
- You’re waking at night because of the pain
- You’ve noticed weakness when lifting or reaching
- You can’t do normal daily activities—dressing, driving, working overhead
- You’ve had a fall or sudden injury to the shoulder
- You’re a sportsperson with a shoulder injury affecting your training
At Phoenix Physio Aylesbury, our chartered physiotherapists specialize in musculoskeletal shoulder conditions. We provide a thorough clinical assessment, clear diagnosis, and a bespoke rehabilitation program—whether your rotator cuff needs gentle progressive loading, sports-specific strengthening, or post-surgical rehab.
Don’t put it off. Rotator cuff injuries that are caught early and treated correctly have the best chance of full, lasting recovery. The shoulder you fix today is the shoulder that carries you through tomorrow.
Conclusion
A rotator cuff injury isn’t something you “wait out.” It’s one of the most common causes of shoulder pain in the UK — and when it’s managed early and correctly, recovery is straightforward. When it’s ignored, it turns into months of pain, weakness, and limited movement.
The reality is simple. Most rotator cuff problems don’t need surgery. They need the right diagnosis, the right exercises, and consistency. Whether it’s tendinopathy, impingement, or even a partial tear, structured physiotherapy remains the most effective path back to full function.
If you’re in Aylesbury and your shoulder pain has been lingering, worsening at night, or affecting your daily activities, don’t leave it to chance. The longer it goes on, the more complex it becomes.
At Phoenix Physio, we focus on clear answers and practical solutions — not guesswork. You’ll know exactly what’s wrong, how long recovery will take, and what to do step by step.
Fix it early, and you stay in control. Leave it too long, and it controls you.